
Case Report | DOI: https://doi.org/10.31579/2641-8975/004
*Corresponding Author: Clarissa Lilli, University of Pittsburgh Diabetes Institute, USA.
Citation: Christine Ngaruiya, Hussein Abubakar, Dorcas Kiptui, Utilization of GTSN improved glycemic control and elevated GLP-1 release compared to a healthful breakfast food (oatmeal) and breakfast skipping without negatively impacting appetitive response or energy intake,DOI: 10.31579/2641-8975/004
Copyright: © 2018 Clarissa Lilli. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 13 February 2018 | Accepted: 22 February 2018 | Published: 28 February 2018
Keywords: Type-2 diabetes, diabetes specific formula, glucose control, GLP-1, breakfast
Background: For people with type 2 diabetes mellitus (T2DM), the frequency and/or composition of the morning meal may be especially important as the disease associated hormonal and metabolic perturbations contribute significantly to poor glucose control and weight gain. Few well-controlled studies have evaluated the effects of skipping breakfast and nutrient composition on metabolic outcomes in T2DM. This study evaluated the impact of consuming one of two convenient and healthful breakfast options versus skipping breakfast on postprandial blood glucose, insulin, glucagon-like peptide-1 (GLP-1), total energy intake and appetite.
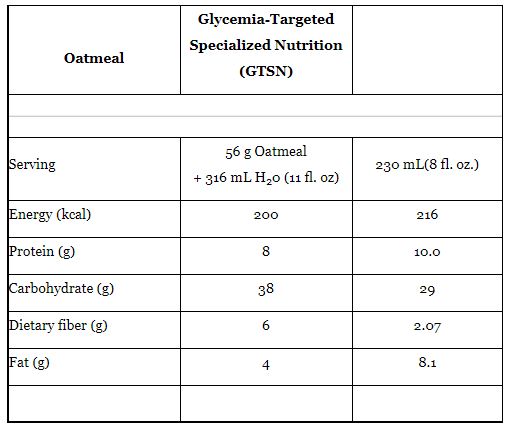
Materials and methods: This was a randomized, controlled, non-blinded, three- treatment, crossover study conducted at two sites. All subjects (n=32) had T2DM. On study day mornings, fasted subjects consumed each test meal in random order: the two nutritional interventions administered were (1) a typical whole food breakfast meal consisting of oatmeal (OAT; 200 kcals, 8g protein, 36g carbohydrate (CHO), 6g fiber, 4g fat) and (2) a calorically-matched glycemia-targeted specialized-nutrition (GTSN; 216 kcals, 10g protein, 29g CHO, 2g fiber and 8g fat) compared to (3) skipping breakfast (SBF). Blood samples for measurement of plasma glucose, insulin and GLP-1 and appetitive responses were collected at baseline (pre-meal) and after consumption of the test meal over 180 minutes.
Results: Postprandial plasma glucose positive area under the curve (pAUC) mean was significantly reduced by 38% (based on individual percent changes) after GTSN compared to OAT. The SBF had the smallest glucose pAUC mean of all interventions. GLP-1 postprandial pAUC median of individual percent changes was significantly elevated after the consumption of GTSN by 280% compared to OAT and 995% compared to SBF. Subjective hunger pAUC mean was significantly elevated and fullness significantly lower after SBF compared to both the OAT and GTSN. No differences in hunger or fullness were observed between the GTSN and OAT interventions.
Conclusion: This study demonstrated that utilization of GTSN improved glycemic control and elevated GLP-1 levels compared to a healthful breakfast food and breakfast skipping without negatively impacting appetitive response or energy intake. These results suggest that GTSN containing slowly digesting carbohydrates and monounsaturated fatty acids (MUFA) may provide additional metabolic benefits when used as a meal replacement compared to oatmeal and breakfast skipping for people with T2DM.
Medical nutrition therapy is a critical part of globally accepted treatment guidelines for type 2 diabetes mellitus (T2DM) [1-6]. An important feature of these nutrition therapeutic guidelines is attention to type and amount of carbohydrate and calorie control leading to weight management. Randomized controlled trials such as the Look AHEAD trial of over 5000 overweight or obese individuals with T2DM [7,8] demonstrate that convenient, prepackaged low-glycemic meal replacements can increase adherence to lifestyle modification resulting in maintenance of weight loss. In the Look AHEAD trial men and women with type 2 diabetes in the intensive lifestyle intervention group, the meal replacements were recommended to be consumed as the breakfast meal and in place of one daily snack. In a smaller study [9], Chinese men and women with T2DM who were provided a low glycemic diabetes meal replacement to replace high glycemic breakfast food items at the morning eating occasion, had improved metabolic responses and glycosylated hemoglobin (HbA1c) was lower (p<0.001) in the Intervention Group at 12 weeks (-0.6 ± 0.1%) and 24 weeks (-0.8 ± 0.1%). Additionally, both weight and waist circumferences were also improved in the Intervention Group vs. Reference Group. Several others have also demonstrated successful maintenance of weight loss with the consumption of breakfast [10] and by the use of meal replacements at breakfast and lunch eating occasions in obese T2DM patients [11-13].
Glycemia Targeted Specialized Nutrition (GTSN) such as the meal replacements utilized in the LookAHEAD [7,8] and Sun et al.[9], trials have been included as an integral part of a recently published Transcultural Nutrition Algorithm that advocates lifestyle modification as an adjunct to pharmacotherapy [4-6]. GTSN formulas containing low glycemic index and slowly digested carbohydrates were shown to exert better glycemic management as compared to standard formulas [9,14-19] when used as a meal or calorie replacement or as a dietary supplement as part of overall nutritional management of diabetes [reviewed in 16]. However, a comparison of the glycemic response of GTSN to other whole food breakfast choices has not been explored.
The current study was designed to compare the impact of skipping breakfast and a whole food, convenient and healthful breakfast option to a convenient and healthful GTSN on postprandial glycemic, insulinemic, glucagon-like peptide-1 (GLP-1), appetitive responses and total energy intake in people with T2DM.
Study Design and Methods
Human subjects
This was a randomized, controlled non-blinded, three-period, three-treatment, crossover study conducted at two sites in the US. This research was reviewed and approved by an Independent Ethics Committee (Schulmann Associates, IRB, OH). Adult subjects (≥ 18 and ≤ 75 years of age) with T2DM receiving stable doses of oral hypoglycemic medication for at least two months were eligible. Prior to participation in the study, all subjects provided applicable privacy authorization and written informed consent. Additional inclusion criteria were (1) BMI was > 18.5 and &le 35.0 kg/m2, (2) weight stable for the two months prior to the screening visit, (3) male or a non-pregnant, non-lactating female, at least 6 weeks postpartum prior to screening visit, (4) if on a chronic medication such as an anti-hypertensive, lipid-lowering, thyroid medication or hormone therapy, the dosage was constant for at least two months prior to screening visit, (5) willingness to follow protocol as described, including consumption of study product per protocol and completing any forms needed throughout the study, (6) at least a two week wash-out period between completion of a previous research study that required ingestion of any study food or drug and their start in the current study. Subjects were excluded from the study if one of the following conditions existed: (1) screening HbA1c level ≥ 9% (as assessed by capillary measurement via A1cNow+®, Bayer, Healthcare, Berlin, Germany) ; (2) use of exogenous insulin or GLP-1 agonists for glucose control; (3) confirmed type 1 diabetes and/or had history of diabetic ketoacidosis; (4) current infection (requiring medication), inpatient surgery or received systemic corticosteroid treatment (with the exception of inhaled (includes nasal), topical, and ophthalmic steroids) in the last 3 months; or received antibiotics in the last 3 weeks; (5) active malignancy (excluding the following dermal malignancies: basal cell carcinoma, squamous cell carcinoma, carcinoma in-situ of the cervix); (6) significant cardiovascular event within 6 months prior to study entry or history of congestive heart failure; (7) end stage organ failure (such as end stage renal disease) or was post organ transplant; (8) history of renal disease; (9) current hepatic disease; (10) history of severe gastroparesis; (11) a chronic, contagious, infectious disease, such as active tuberculosis, Hepatitis B or C, or HIV; (12) taking any herbals, dietary supplements, or medications, other than anti-hyperglycemic medications, during the past four weeks prior to screening visit that could profoundly affect (in the opinion of the primary investigator) blood glucose; (13) clotting or bleeding disorders (the use of Plavix® or a similar anticoagulant drug with no reported difficulty during blood draws was allowed); (14) allergic or intolerant to any ingredient found in the test meals; (15) habitual use of tobacco products (e.g. cigarettes, pipes, chewing tobacco) or (16) participant in another study that has not been approved as a concomitant study by AN.
Subjects were excluded from the analysis if they (1) did not meet eligibility criteria; (2) have a missing positive AUC for plasma glucose concentration over 0 -180 minutes (from the meal tolerance test (MTT)); (3) did not consume all of the test breakfast or lunch meal, including required beverage, within the allotted time.
Three treatments were assessed in random order and were comprised as follows: skipped breakfast (SBF; 12 fl oz compulsory beverage), oatmeal (OAT; unflavored, unsweetened instant oatmeal {prepared with 1-1/3 cups (316 mL) water and microwaved 2-3 minutes per manufacturer's instructions; The Quaker Oats Company, Chicago, Illinois} + 12 fl oz of compulsory beverage) or 1 serving of the GTSN (Glucerna Triple Care {8 fl. oz., Abbott Nutrition, Columbus, Ohio} + 4 fl oz compulsory beverage). The compulsory beverage was decaffeinated coffee/ tea or water and up to 4 packets of non-caloric sweetener per each subject's preference. Compulsory beverage choice, sweetener usage and total beverage consumption (12 fluid ounces total) was constant for a given subject across all three treatments. Macronutrient composition was similar between the two caloric meals (Table 1).
Study procedures
Eligible subjects were scheduled to report to the study site on three separate mornings after a 8-14 hour overnight fast, with 7-14 days between study visits. During study visits, subjects' medications were reviewed to ensure no changes in hypoglycemic agents and study preparation procedures were documented. Study procedures were similar to those of a standard oral glucose tolerance test [20]. However, postprandial response to a mixed meal or meal skipping was assessed instead of a glucose load. Study preparation required the study subjects to (1) consume at least 150 g of carbohydrate during the 3 days prior to the study visit, (2) refrain from vigorous physical activity the day before the study visit, and (3) consume the provided snack (180- 200kcal; 5-8 gram fat7; 20-24 grams carbohydrate; 12–16 grams protein) between 8-10 pm the evening before the visit.
Upon arrival to the study visit, the subject's capillary blood glucose level was obtained to confirm appropriate fasting and if the level was ≥ 60 and < 300 mg/dL, the subject was allowed to continue with study procedures. In the event that capillary blood glucose was not within the specified range, the subject was required to exit the study. All subjects consumed each of the three treatments per the randomization schedule within 10 minutes and the first intake of food/beverage was set to be time zero. Blood samples for plasma glucose (Glucose hexokinase, UV, Roche Hitachi Modular), serum insulin (Immunometric assay, Siemens Healthcare Diagnostics IMMULITE Series), and plasma GLP-1 (7-36 amide collected in dipeptidyl peptidase-IV containing vaccutainer, ELISA from ALPCO™ Immunoassays, Salem, NH) were obtained at baseline (right before meal consumption), and postprandially at 30, 60, 90, 120, and 180 minutes (± 5 min). All blood analyses were performed at a central laboratory (ICON Central Laboratories, Farmingdale, New York).
Subjective appetitive responses via 100 mm line visual analog scales were obtained in conjunction with each blood sampling time (± 10 min). Appetitive questionnaires for the six modalities were anchored with the descriptive terms "not at all" and "extremely" for hunger, fullness, desire to eat, thirst and nausea whereas "nothing at all" and "a large amount" were the descriptive anchors for prospective consumption.
Statistical analysis and Calculations
The methodology for measuring glycemic response was adapted from previous studies [20,21]. The primary variable was the positive area under the curve (pAUC) for plasma glucose concentration over 0 to 180 minutes. The power calculation was based on a 20% reduction of the GTSN pAUC compared with the pAUC from the control in this study (OAT). Assuming a 30% attrition rate, and keeping the number of subjects enrolled as a multiple of 6 for equal treatment sequence assignment, 36 subjects were targeted for enrollment. Sample size was determined using nQuery Advisor® Release 5.0. The primary statistical analysis was on the protocol evaluable data set. Data are presented as Least Squares Means ± SEM for repeated measures analysis of variance (ANOVA). Statistical analyses were performed using three-treatment, three-period, repeated measures ANOVA with site, treatment and period as fixed effects and subject as random effect. If this test was determined to be inappropriate due to non-normality, then three pairwise treatment differences were analyzed using signed rank tests.
Calculations for area under the curve from 0-180 minutes (AUC0-180 min), positive AUC0-180 min, peak value, adjusted peak value, and peak time, were completed for glucose, insulin, and GLP-1. These calculations were performed according to a priori rules, described briefly here. AUC was calculated by the trapezoidal method for each variable. Positive AUC0-180 min was also calculated using the trapezoidal method for only those values that were above the baseline (time 0) value for a given variable and any values that were below baseline were considered as zero. Peak value was the maximum value of all valid points over 0-180 minutes. Adjusted peak value was the peak value minus the value at t = 0. Peak time was the first time point during the 0-180 minute interval at which the peak value was attained.
Subjects
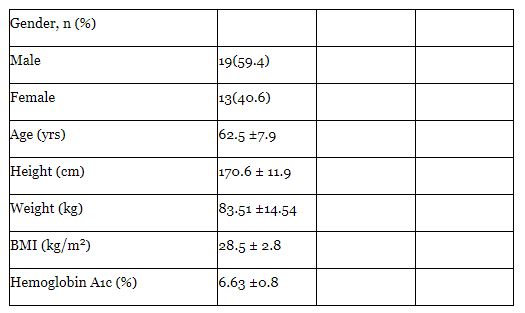
Thirty-seven subjects signed informed consent forms and were enrolled into the study. However, five were not included in the protocol evaluable analysis due to the following reasons: one subject had a missing value for primary variable, the same subject plus four others did not consume the experimental beverage/ meal within the allotted time and two of these voluntarily withdrew from the study. Demographic information and baseline characteristics of the 32 evaluable subjects are presented Table 2.
Plasma Blood Glucose
There were no differences observed for baseline plasma glucose among the treatments (137 ± 5 mg/dL for OAT; 133 ± 5 mg/dL for GTSN; 137 ± 5 mg/dL for SBF). The adjusted plasma glucose values over the postprandial time-points indicated a differential response among the three treatments, as can be seen by the separation of the median adjusted glucose response curves (Figure 1a). This visual difference was confirmed by assessing the glucose pAUCs for each treatment where GTSN elicited a 38% (based on individual percent changes) lower pAUC than OAT (GTSN 4119 ± 461 (mg/dL)*min) compared to OAT 7531 ± 461(mg/dL)*min; repeated measures ANOVA; p < 0.0001; (Figure 1b). As expected the SBF treatment resulted in the smallest pAUC (437 ± 460 (mg/dL)*min), due to the lack of caloric delivery. The peak plasma glucose (OAT 214 ± 7 mg/dL; GTSN 178± 8 mg/dL; SBF 142 ± 7 mg/dL; p < 0.0001 for each pairwise comparison) and adjusted peak plasma glucose (OAT 76± 4 mg/dL; GTSN 46 ± 4 mg/dL; SBF 5 ± 4 mg/dL; p < 0.0001 for each pairwise comparison) response was found to be significantly different among all three treatments, with OAT eliciting the highest mean plasma glucose value. The mean peak plasma glucose response observed one hour after consumption of GTSN met the postprandial blood glucose of < 180mg/dL per ADA recommendations [3]. This was not observed from the other caloric treatment, OAT.

Plasma Blood Glucose
Glycemia-targeted specialized-nutrition has been demonstrated to provide metabolic benefits for people with diabetes as compared to standard nutritional formulas for glycemic control, GLP-1 response and weight loss [9,16- 19,22]. The current study is the first to indicate that GTSN formulas exert significantly lower postprandial glucose response as compared to a whole food breakfast (oatmeal) in people with T2DM. This finding emphasizes the impact of breakfast choice on postprandial glycemic excursions. The two caloric interventions in this study provided different amounts of total and available carbohydrate (available CHO = total CHO – fiber). GTSN supplied 29 g total CHO and 27 g available CHO whereas OAT provided 38 g total CHO and 32 g available CHO. Providing lower total and available CHO contributes to the GTSN eliciting a lower glycemic response. Additionally, the GTSN consisted of a blend of slowly-digested, slowly-absorbed CHO sources which result in blunted glycemic response [22], while those carbohydrates in the OAT product are not specialized for this purpose.
Glycemic control can also be impacted by the mere act of consuming breakfast. In people with T2DM, post-breakfast hyperglycemia has been shown to occur more frequently than after other eating occasions, despite treatment with anti-hyperglycemic medicines/ insulin [23]. This observation may lead people with T2DM to skip breakfast in an attempt to control this phenomenon. In this study the absence of postprandial glycemic response observed when breakfast was skipped must be considered with caution. Studies clearly show that skipping breakfast exerts noted metabolic consequences such as a strong association with impaired fasting glucose [24] and lipids, a reduced postprandial insulin sensitivity in healthy obese women [25], and is the primary cause for hypoglycemia [26]. Further, breakfast skipping is positively associated with being overweight or obese from cross-sectional studies conducted in the US, Eastern Mediterranean, Taiwan and Asian/ Pacific regions [27-30].
Breakfast choices [26], as well as all food choices at all eating occasions that minimize postprandial hyperglycemia are important for reducing the risk of developing diabetes related micro- and macrovascular complications in individuals with type 2 diabetes [31,32]. To facilitate appropriate food choices that impart glycemic control and support weight management goals, medical nutritional therapy consisting of GTSN is often recommended and utilized in parallel with pharmacotherapy. However, diabetes dietary guidelines can be cumbersome. Due to their ease of use and previously discussed efficacy, meal or calorie replacements that are also glycemia-targeted have been incorporated as a recommended tool in several diabetesspecific nutritional plans [33,34] and within the recently published Transcultural Diabetes-specific Nutritional Algorithms [4-6]. This study demonstrates that breakfast consumption in people with T2DM can be metabolically beneficial when appropriate glycemia-targeted breakfast choices are made and supports the use of GTSN at the breakfast eating occasion as recommended in the Transcultural Diabetes-specific Nutrition Algorithms [4-6].
Plasma GLP-1 and Serum Insulin
GLP-1 secretion by the L-cells of the intestinal lumen is stimulated by carbohydrate, protein and fat ingestion [35]. This hormone has a demonstrated role in inhibition of gastric acid secretion and gastric motility as well as enhancement of satiation [35]. The current research supports previous findings showing postprandial GLP-1 secretion in people with diabetes is elevated by the consumption of GTSN [18,19,22]. However, this study is the first to compare GLP-1 response after GTSN consumption compared to a whole food and breakfast skipping. The elevation in GLP-1 after eating is not unexpected, as it is known that GLP-1 secretion is directly related to macronutrient composition, specifically carbohydrate [36] and gastric distention (imparted by ingestion of a larger volume of food). However, the higher carbohydrate, larger volume treatment (OAT) neglected to elicit GLP-1 release equal to or greater than the lower carbohydrate, smaller volume GTSN. This differential response despite protein and energy matching with both carbohydrate content and volume favoring the OAT provision aligned with previous work indicating that the type of carbohydrate [18,19,22] and monounsaturated fatty acids (MUFA) [37] are important for GLP-1 release in people with diabetes. Since the largest GLP-1 response was observed after the consumption of GTSN which had 9 g less total carbohydrate and 3.9 g more total fat (including MUFA) than OAT, is it suggestive that the slowly digesting, low glycemic carbohydrate blend and monounsaturated fat blend in GTSN plays an important role for GLP-1 response. This conclusion is supported by previous work that demonstrates slowly-digested carbohydrate and MUFA fat containing formulations of GTSN elicit a larger GLP-1 response compared to GTSN without slowly digesting carbohydrate [19] and a standard oral nutritional 18,22].
Furthermore, despite GTSN eliciting similar postprandial serum insulin pAUC compared to OAT the incretin effect of GLP-1 appeared to be maintained. The peak and adjusted peak insulin levels reached after consumption of GTSN were higher than after OAT.
Subjective Appetitive Response and Energy Intake
Physiologically, the consumption of breakfast has been associated with satiation and satiety [38], decreased body weight [39,] and decreased risk for diabetes and CVD [40,41]. As expected, skipping breakfast resulted in the highest hunger and least fullness which were significantly different from the caloric treatments. However, the hunger and fullness observed from the skipped breakfast did not elicit acute changes in energy intake. This is likely due to the compulsory lunch meal consumed at the end of the meal tolerance test (which could not freely differ between treatments) thus leaving only the evening meals and snacks (if consumed) available for energy compensation. Subjective appetitive responses and total daily energy intake were similar after consumption of GTSN and OAT suggesting the similar impact on satiation and supporting the subsequent
Study limitations
The study limitations include the acute nature of the study treatments, thereby eliminating the extrapolation to more chronic and weight related outcomes. As such future work should characterize chronic outcomes and take into account the possibility of fatigue in regard to GTSN consumption by offering a variety of flavor options.
This research demonstrated that the utilization of GTSN improved glycemic control and elevated GLP-1 release compared to a healthful breakfast food (oatmeal) and breakfast skipping without negatively impacting appetitive response or energy intake. As this study was acute, it is recommended that future work assess similar outcomes over a prolonged ingestion period and potentially at different eating occasions. The current findings suggest that glycemia-targeted specialized nutrition containing slowly digested carbohydrates and MUFA provides unique metabolic benefits for people with T2DM when used as a meal replacement and are appropriate for incorporation into diabetes treatment algorithms.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
